Understanding Flat-Head (Deformational Plagiocephaly) and What You Should Know
What Is Deformational Plagiocephaly?
Deformational plagiocephaly (often called “flat-head syndrome” or "positional plagiocephaly") is when an infant develops flattening on one side or at the back of the skull due to external pressure. Because infant skull bones are soft and malleable, persistent positioning (especially favouring one side) can lead to asymmetries of the head, ears, or face.
Risk factors include:
- Neck tightness or asymmetry (such as torticollis) causing the baby to turn the head more one way.
- Prolonged time in one position (e.g. sleeping, car seats, swings).
- In utero constraints, birth trauma, multiple births, or being born breech.
- Being an early infant (younger than 6-months) since bones are more pliable and the skull is growing fastest then.
Recent Research Insights: What Do We Know Now?
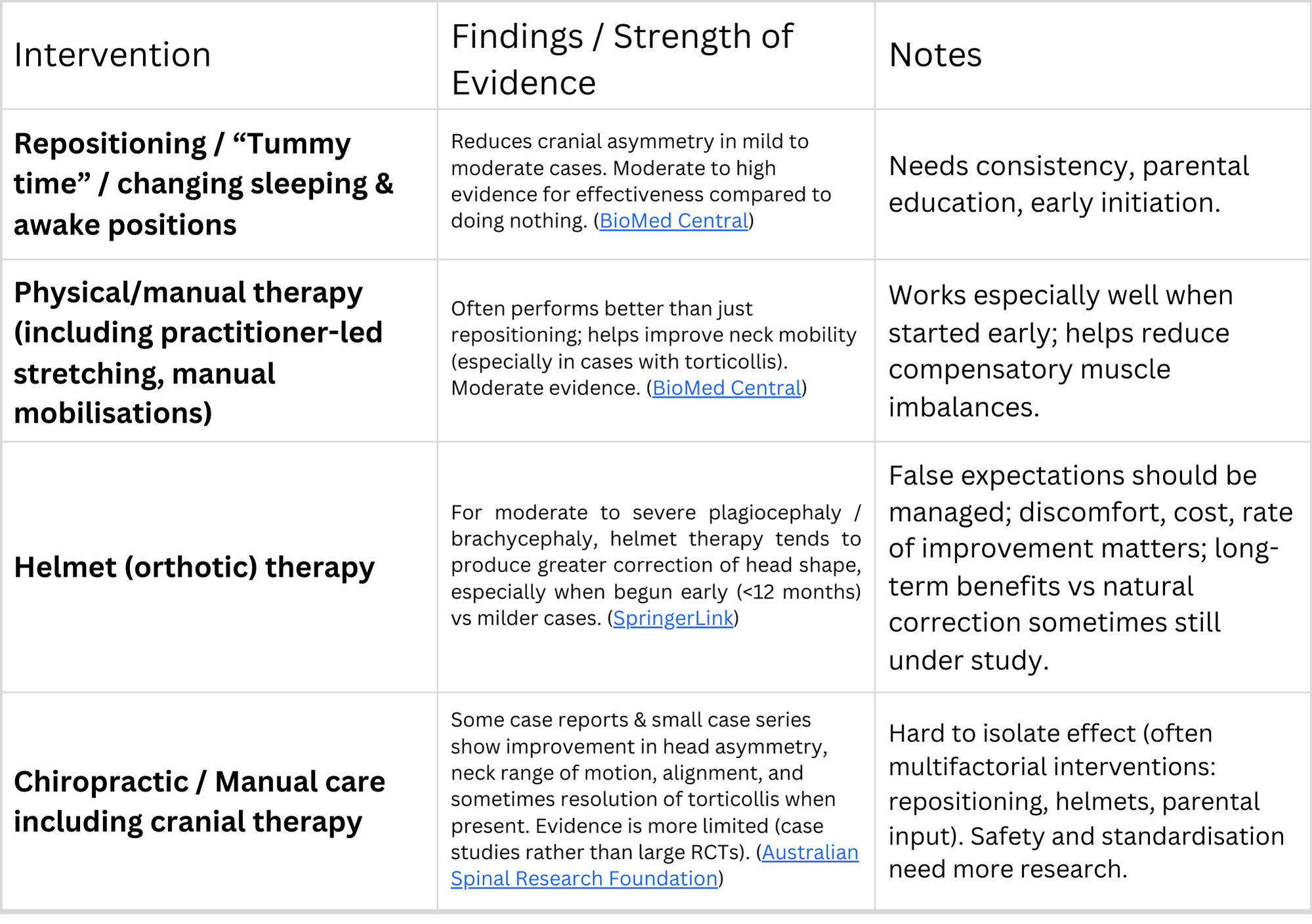
There is growing research into how various non-surgical, conservative interventions can help with plagiocephaly. While the evidence is still limited in quality in some areas, several findings are emerging (See chart):
Recent systematic reviews suggest that while repositioning and physical therapy are low risk and helpful, especially in mild-to-moderate cases, they may not always match the greater improvements seen with helmets in more severe cases.
Can Chiropractic Really Help?
Chiropractic or manual care may play a supportive role in certain circumstances. Some of the ways it may help:
Improving neck mobility / treating torticollis: If the infant is favouring one side because of tight neck muscles or restricted motion, manual therapy (including chiropractic adjustments, stretching, mobilisations) can help balance neck motion. Improved neck movement allows more opportunity to reposition the head and reduce external pressure.
Cranial asymmetry: There are case reports showing head shape improvements in infants receiving manual therapy plus repositioning, and sometimes helmet therapy. For example, a case report showed a decrease in cranial vault asymmetry index (CVAI) from ~14.3% to ~5.8% with combined care (manual + helmet).
Early age is important: The younger the infant (especially under 6 months), the more likely to see more significant head shape improvement. After a certain age, skull bones become less pliable and shape correction becomes more difficult.
However, important caveats:
There is no guarantee of full correction, especially in moderate to severe cases, or if intervention starts late.
Effects are often modest unless intervention is comprehensive (including repositioning, physical therapy, parental participation, possibly helmet) and consistent.
More high-quality studies (randomised controlled trials) are needed to better understand exactly what chiropractic/manipulative techniques work, how often, safely, and how they compare or combine with established methods.
What You Can Do: Practical Takeaways for Parents
Early assessment: If you notice a flat spot or your baby favouring looking one way, it’s worth having them assessed early (ideally before 6 months). The sooner interventions begin, the better the potential outcome.
Repositioning & “tummy time”: Make sure supervised tummy time, alternating head and body positions, limiting time in car seats and carriers where head rests the same way—these are simple, low-risk things that help.
Physical/manual therapy / chiropractic care: If there is neck tightness (torticollis) or restricted motion, getting help from a professional (physio, manual therapist, chiropractor) may help. These practitioners can use gentle techniques, stretches, adjustments.
Helmet therapy: For more severe deformities, or when repositioning/manual methods aren’t sufficient, helmets may be recommended. Understand the commitment (time worn, cost, follow-ups), and weigh against expected benefit.
Monitoring: Track progress over time (measurements or photos), watch motor development and head shape, get regular follow-ups.

What We Do at Adelaide Family Chiropractic
- Assess neck range of motion, head shape, and movement preferences.
- Provide gentle chiropractic/manual care to address neck restrictions.
- Guide parents with positioning, tummy time, home exercises.
- Work with helmet therapy providers when needed (for moderate/severe cases).
What to Expect
- More change if started earlier (under 6-months)
- Regular sessions over weeks to months might be required
- Improvements in head shape are more likely when combined with repositioning and parental compliance
- If your baby is older or the deformity is more severe, correction may be partial but should still reduce asymmetry and improve function
If you’d like to talk about your baby’s head shape, feel free to contact us. We can set up a thorough assessment and figure out a plan together.
Contact UsReferences:
Ellwood, J., Draper-Rodi, J. & Carnes, D. The effectiveness and safety of conservative interventions for positional plagiocephaly and congenital muscular torticollis: a synthesis of systematic reviews and guidance. Chiropr Man Therap 28, 31 (2020). https://doi.org/10.1186/s12998-020-00321-w
Corte, A.D., Rohde, M.A. Use of orthotic helmets in children with positional plagiocephaly and brachycephaly: a systematic review. Childs Nerv Syst 41, 163 (2025). https://doi.org/10.1007/s00381-025-06826-0
Doyle M. Improvement in plagiocephaly, cervical range of movement, primitive reflexes, and subjective parental feedback in an infant co-managed with chiropractic care and helmet therapy: a case report and review of the literature. Asia-Pac Chiropr J. 2020;1.2:online only. URL https://apcj.rocketsparkau.com/plagiocephaly-reduction–doyle/
Hash JL. 2014. Deformational plagiocephaly and chiropractic care: A narrative review and case report, JOURNAL OF CLINICAL CHIROPRACTIC PEDIATRICS Volume 14, No. 2, March 2014. https://jccponline.com/Vol14Issue02.pdf